The first version of the Giv mobile app was built fast to get a startup launched. It looked like an app. It did not work like a tool that a Direct Support Professional would use in someone's home, mid-shift, while providing care. This is the rebuild story.
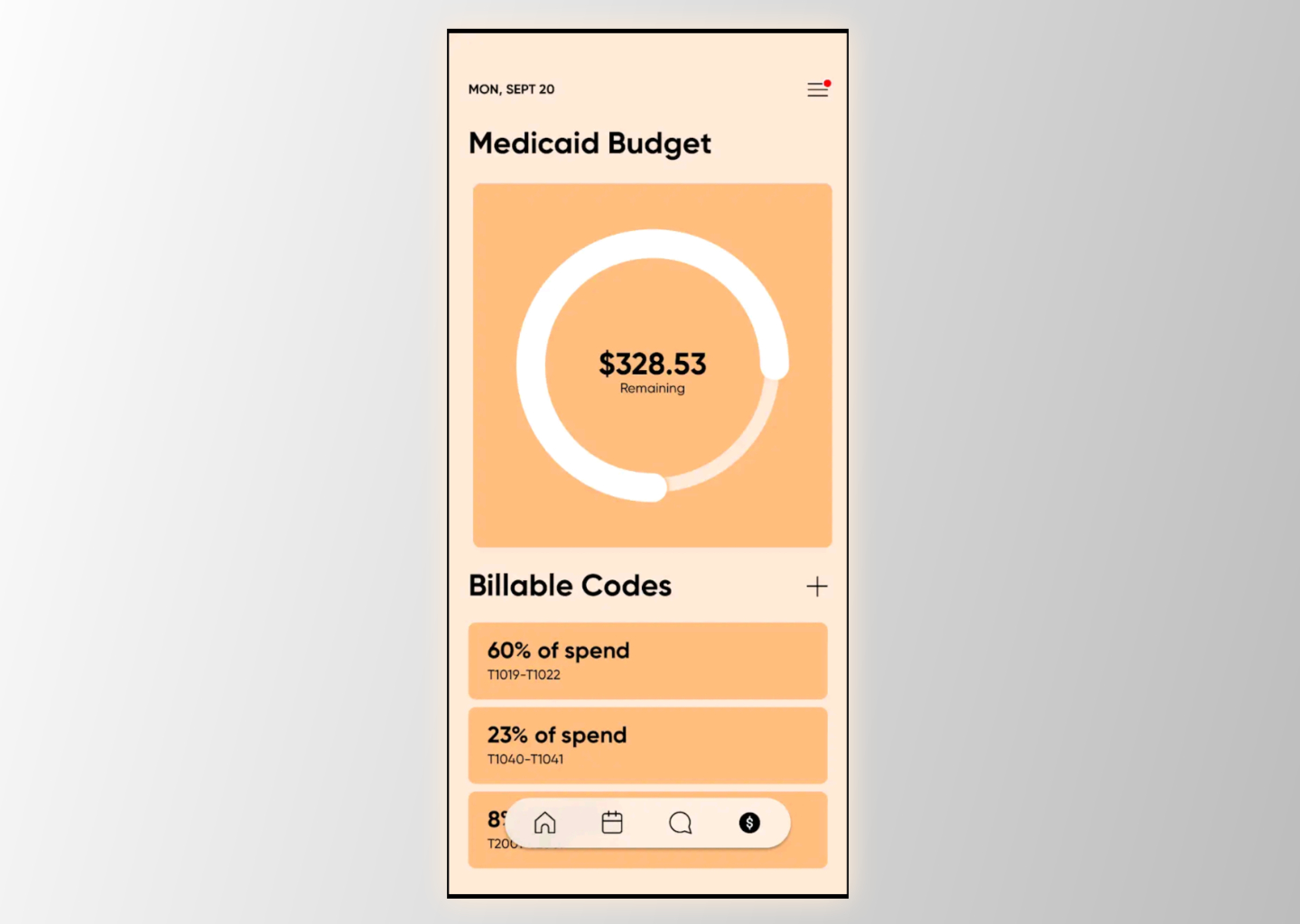
Original MVP
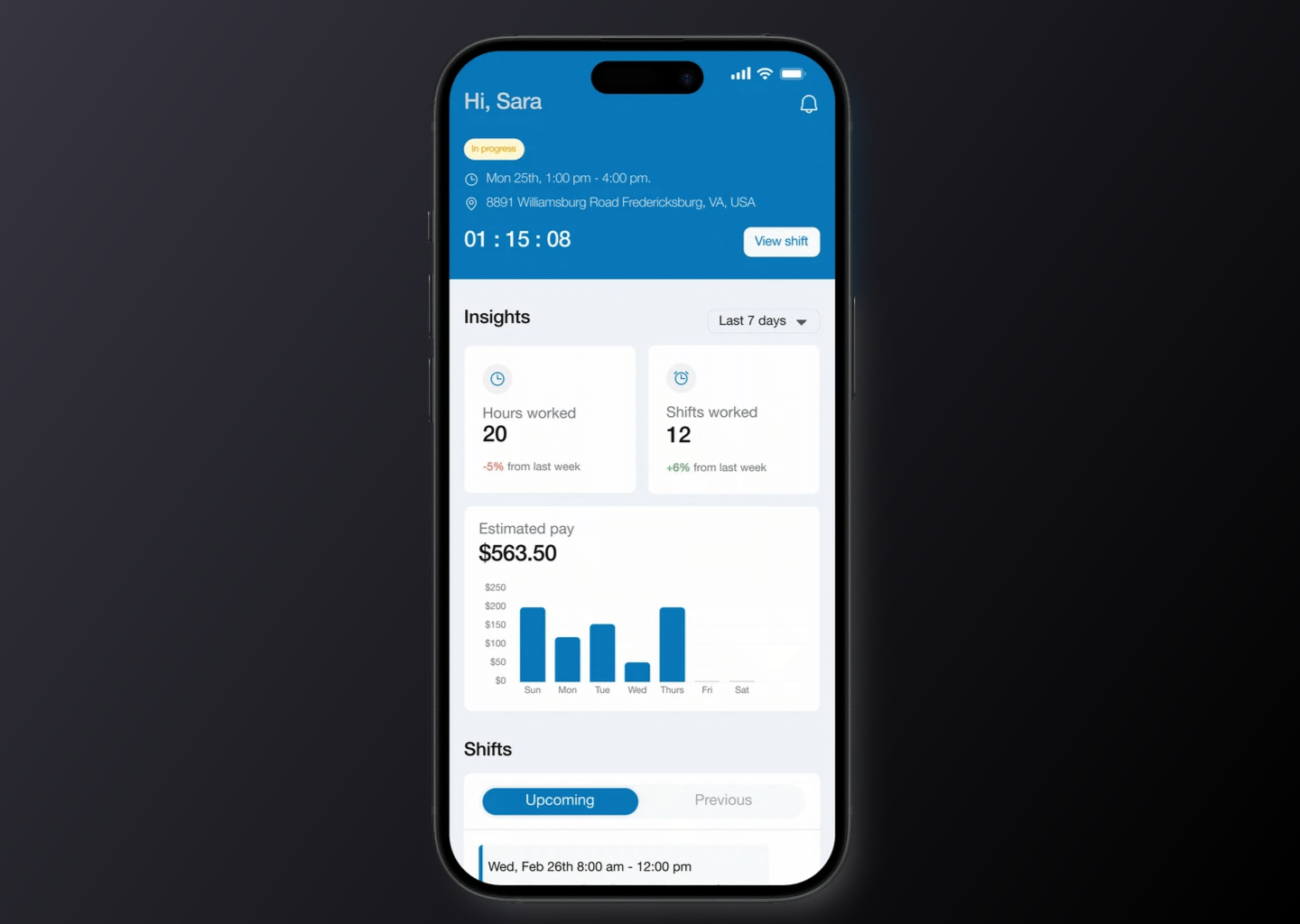
Rebuilt Design
Project Details
- Client: Giv Healthcare
- Role: Lead UX/UI Designer
- Scope: Full app rebuild -- flows, features, interaction design, finished screens
- Platform: iOS and Android (standalone mobile app)
- Users: Direct Support Professionals (DSPs)
- Related: Healthcare Platform | Billing + Design System
- Live Product: givhealthcare.com/mobile
The Challenge
DSPs -- the caregivers who support people with IDD in group homes, supported living, and community settings -- are not office workers. They are in the field, in clients' homes, moving between tasks. The original mobile app MVP had been built quickly to demonstrate that the product existed. It focused on visual presentation and basic feature coverage, not on the actual context in which a DSP would use it: arriving at a shift, caring for a person, documenting everything that happens, managing medications, and closing out hours -- all from a phone, all while attending to a human being who needed their attention.
Electronic Visit Verification (EVV) -- the federal Medicaid requirement that verifies a caregiver's location at the start and end of each shift -- was a compliance layer that had to be built in without creating friction for DSPs who didn't know why they were being tracked. Medication logging had to be accurate and time-stamped without slowing down a caregiver who was, in that moment, administering a medication to someone in their care. Custom client documentation -- goals, behavioral notes, specific reporting requirements that varied by individual -- had to be surfaced automatically based on who the DSP was working with, not found through navigation. The MVP had none of this figured out at the interaction level. The categories were there. The flow logic was not.
The Strategy
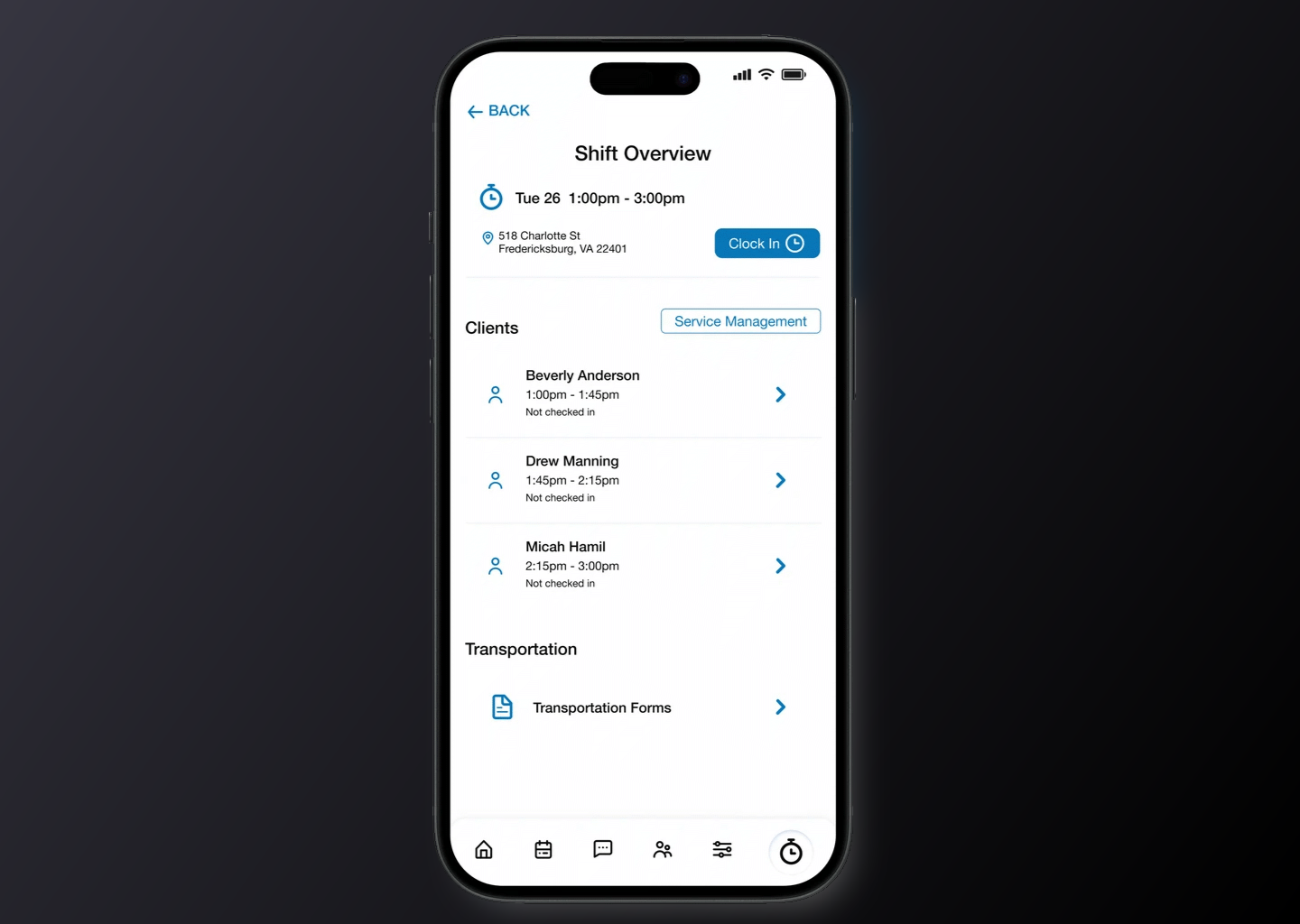
The rebuild started from the actual sequence of a shift. Arrival. Check-in. Client orientation. Service delivery. Documentation throughout. Medication administration. Shift close. Every screen in the rebuilt app was mapped to a specific moment in that sequence. The question for each screen was not "does this feature exist here" but "is this the right moment to surface this information, and is the right action obvious without explanation."
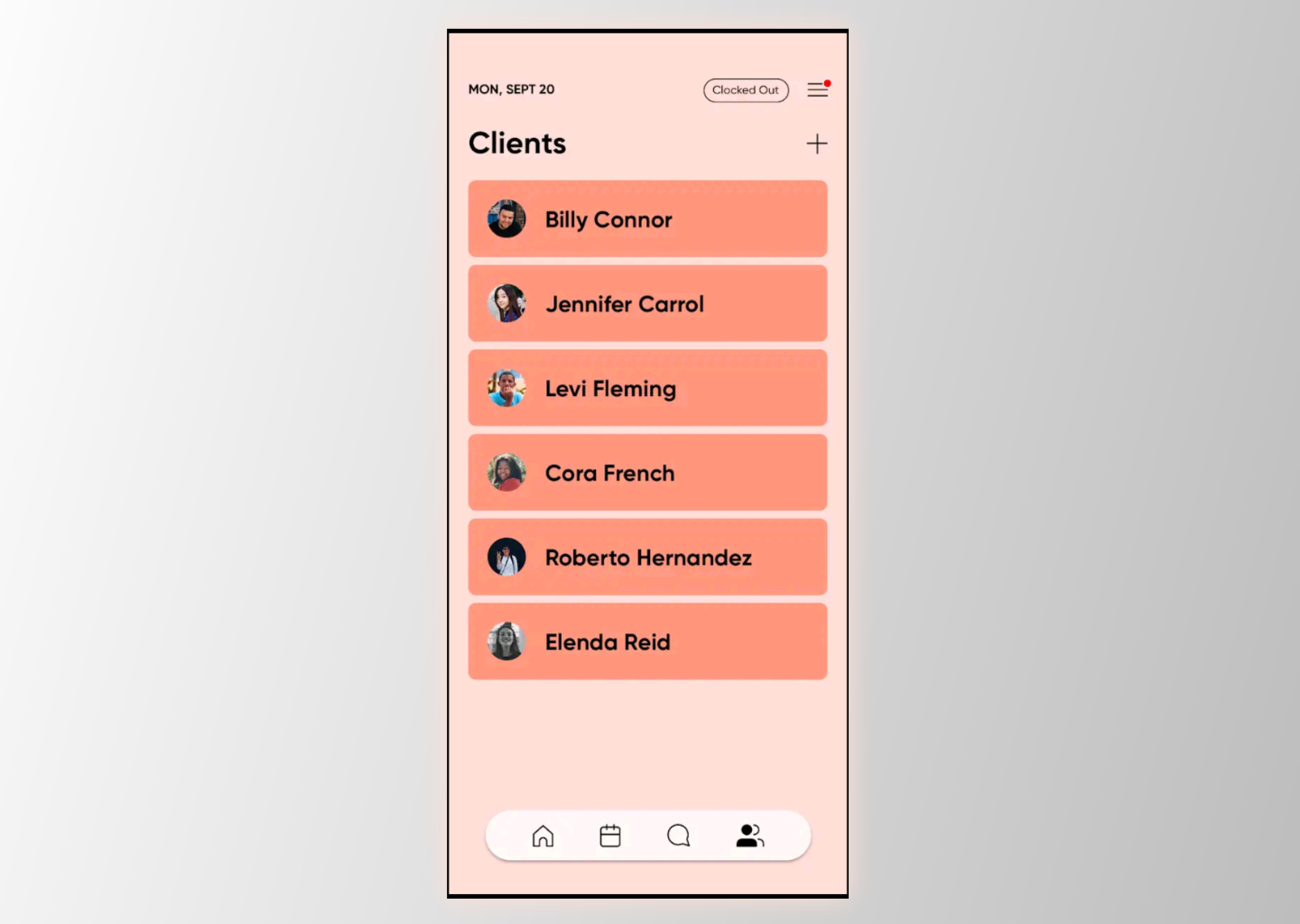
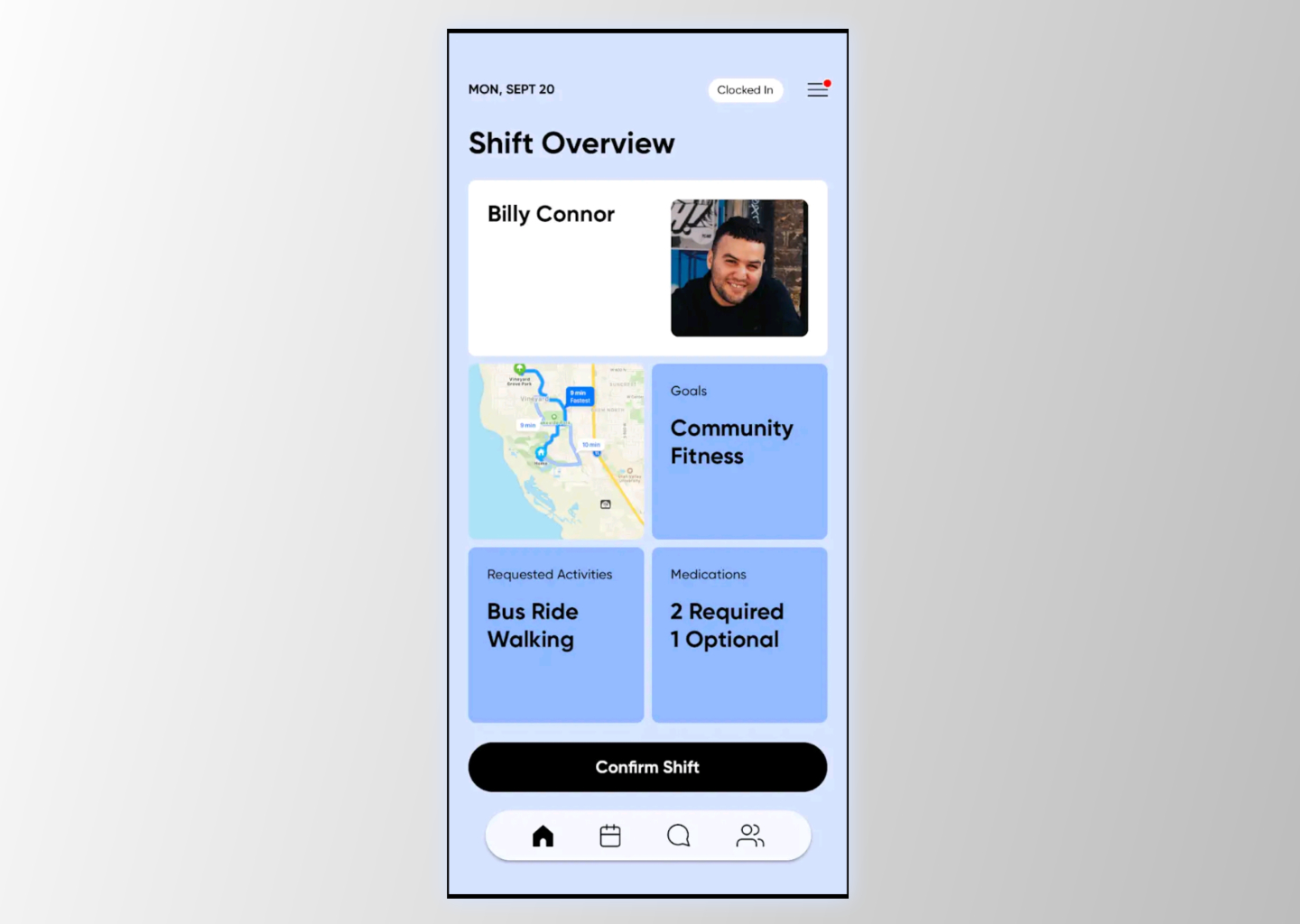
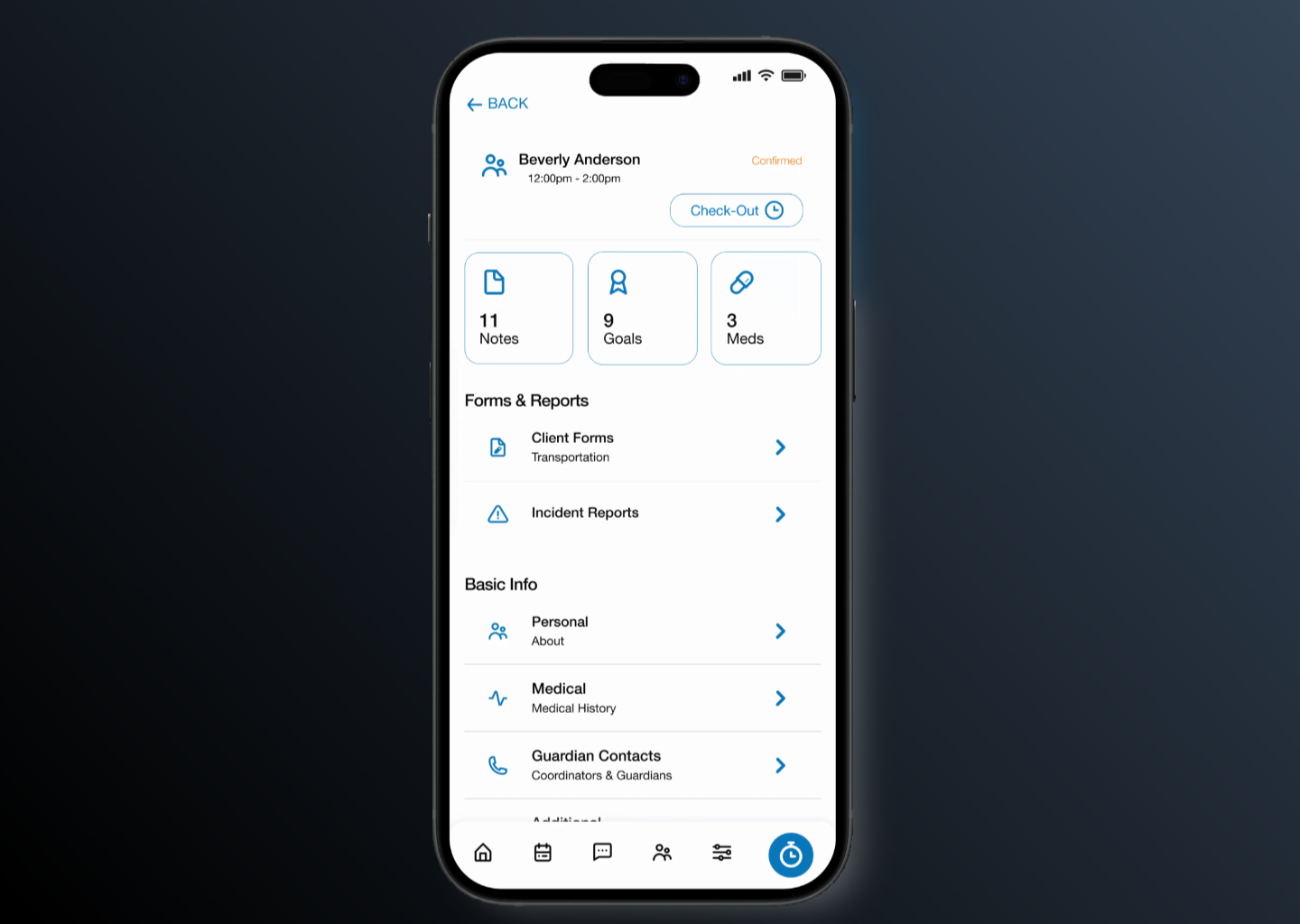
EVV compliance was built into the check-in flow invisibly. The geo-location capture happened as part of shift start -- DSPs confirmed they were starting a shift, and the system handled the federal reporting requirement behind the scenes. The client profile was surfaced at the top of every shift view: who this person is, what their current goals are, what behavioral notes are active, what medications are scheduled. Not in a separate profile tab -- in the shift itself, because that information was relevant precisely at the moment a DSP began their work.
The Execution
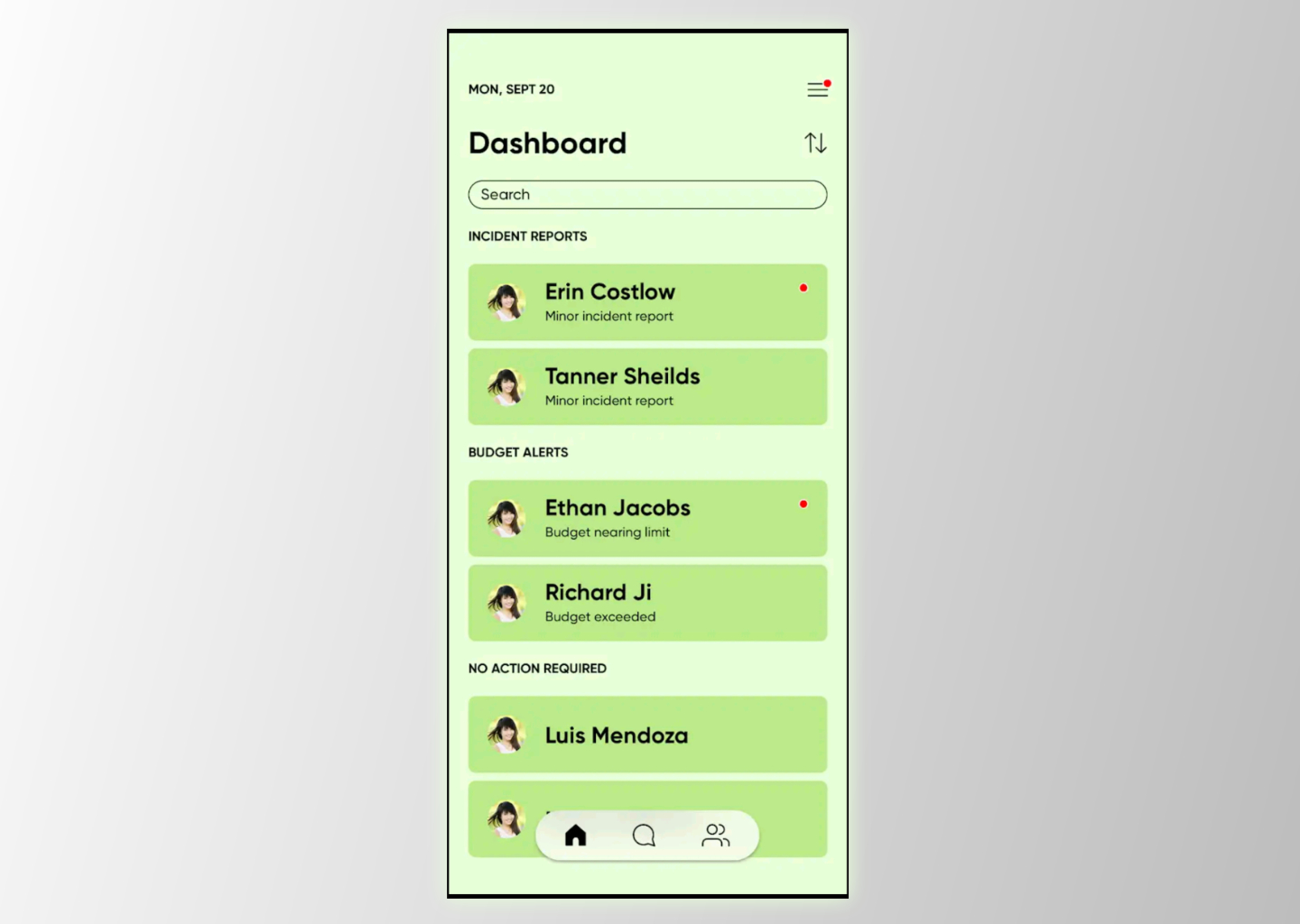
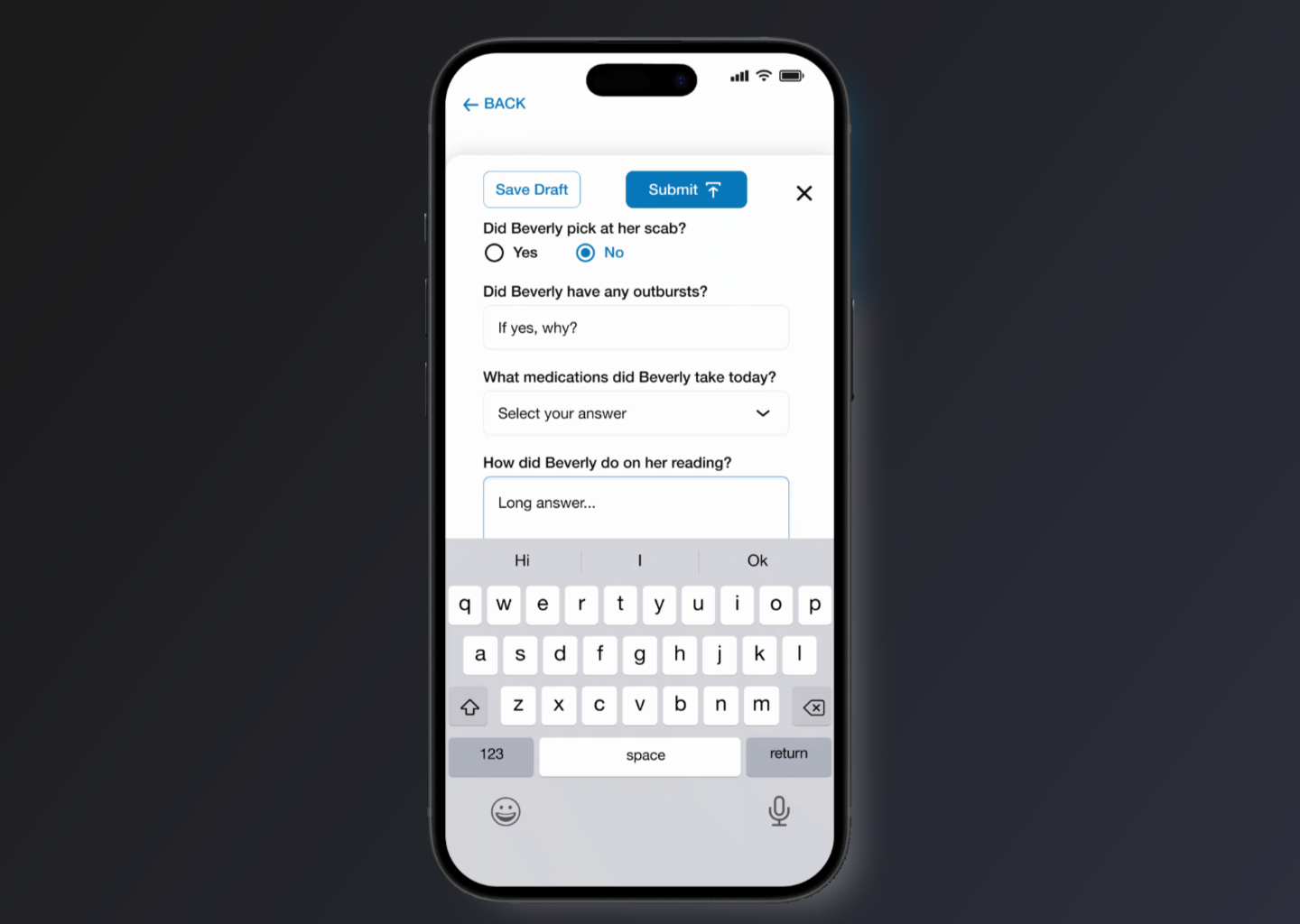
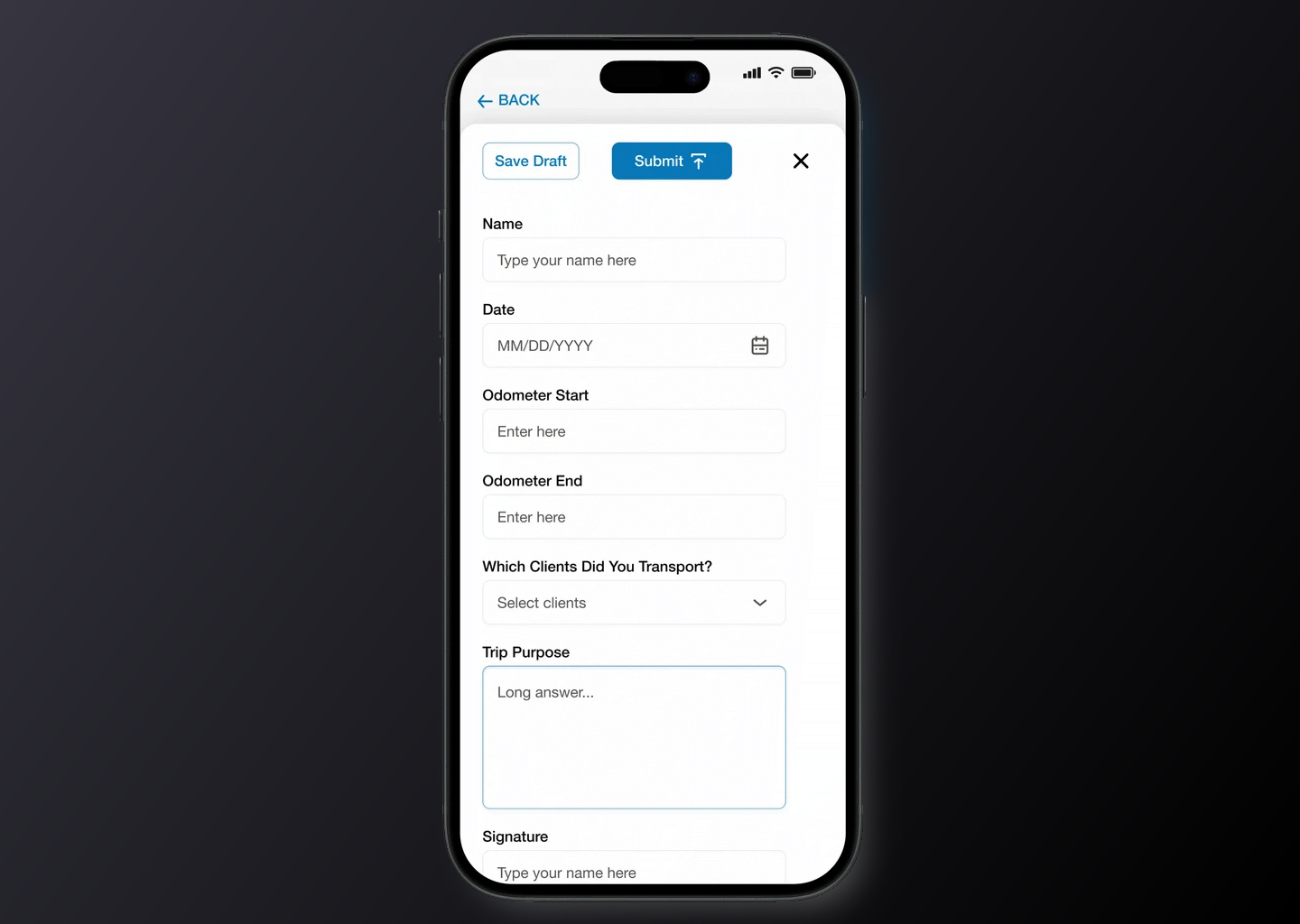
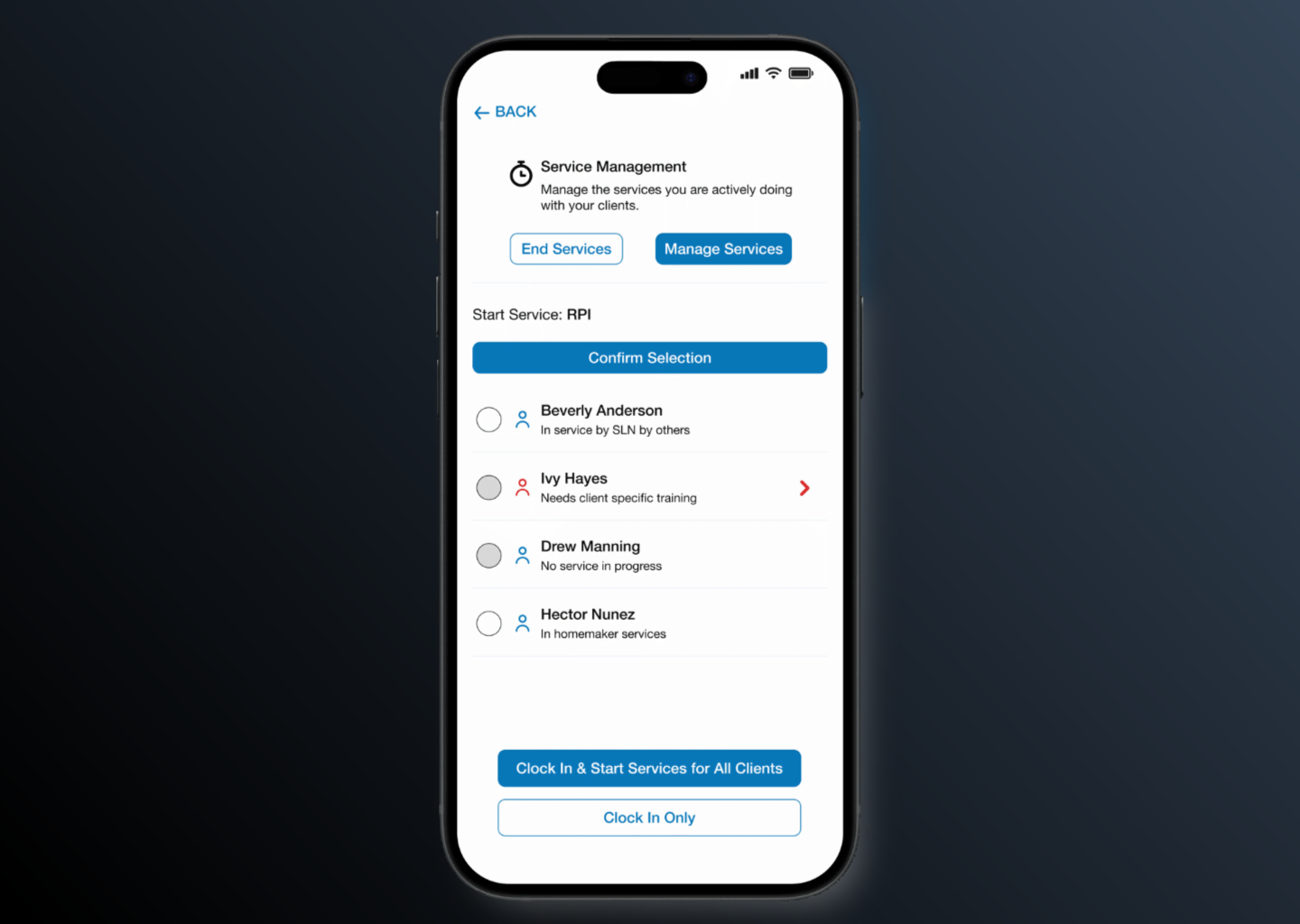
The rebuilt app covered the full shift lifecycle: check-in with EVV, client profile access (medical history, behavioral notes, goals, human rights restrictions), shift notes and custom documentation forms per client, medication logging tied to the electronic medication administration record (eMAR), service code tracking for each activity during a shift, incident reporting, transportation tracking with geo-location for mileage verification and compliance, and caregiver pay and hours stats accessible without requiring a call to the administrative office.
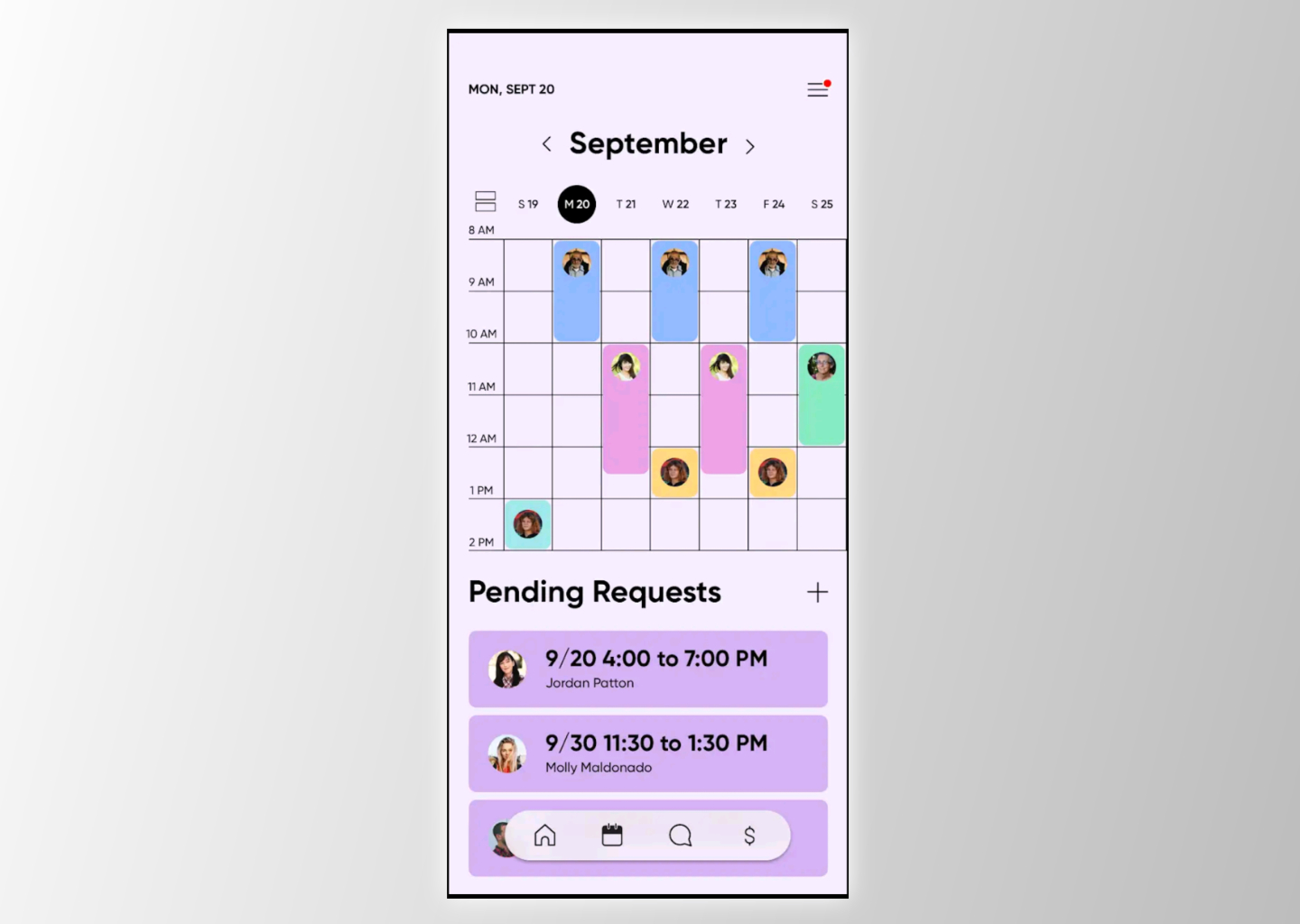
Impromptu shifts -- the unscheduled, last-minute coverage situations that were unavoidable in agencies with high caregiver turnover -- were designed as a first-class feature. Rather than a workaround, the app let DSPs start unscheduled shifts with clients they were approved to work with, while the system automatically enforced training requirements, verified Medicaid budget availability, and ensured documentation standards were met even when the shift wasn't pre-planned. Compliance happened by default, not by memory.
Multi-code service tracking -- the ability for a DSP to log the different service types they provided during a single shift -- was presented in a clean, scannable format that didn't require knowledge of billing codes. The DSP selected what they did; the system mapped it to the correct Medicaid service code for billing.
The Results
The Giv mobile app launched on iOS and Android. The integration with the desktop platform meant that everything a DSP documented in the field -- shift notes, medication logs, service codes, incident reports -- fed directly into the agency's billing and compliance reporting without any manual transfer. The caregiver who arrived for a shift had, on their phone, the same information that had previously required a verbal handoff from the outgoing caregiver or a binder kept at the care site. The agency had compliance documentation generated automatically from the work DSPs were already doing. The knowledge gap that had defined shift handoffs in IDD care had a different shape.