When Giv's CEO decided to build a care management platform for IDD agencies, there was no playbook to follow. No comparable software existed for the space. There was a dev team, a set of real problems that agencies were drowning in, and the first designer hired to figure out what the product should actually be.
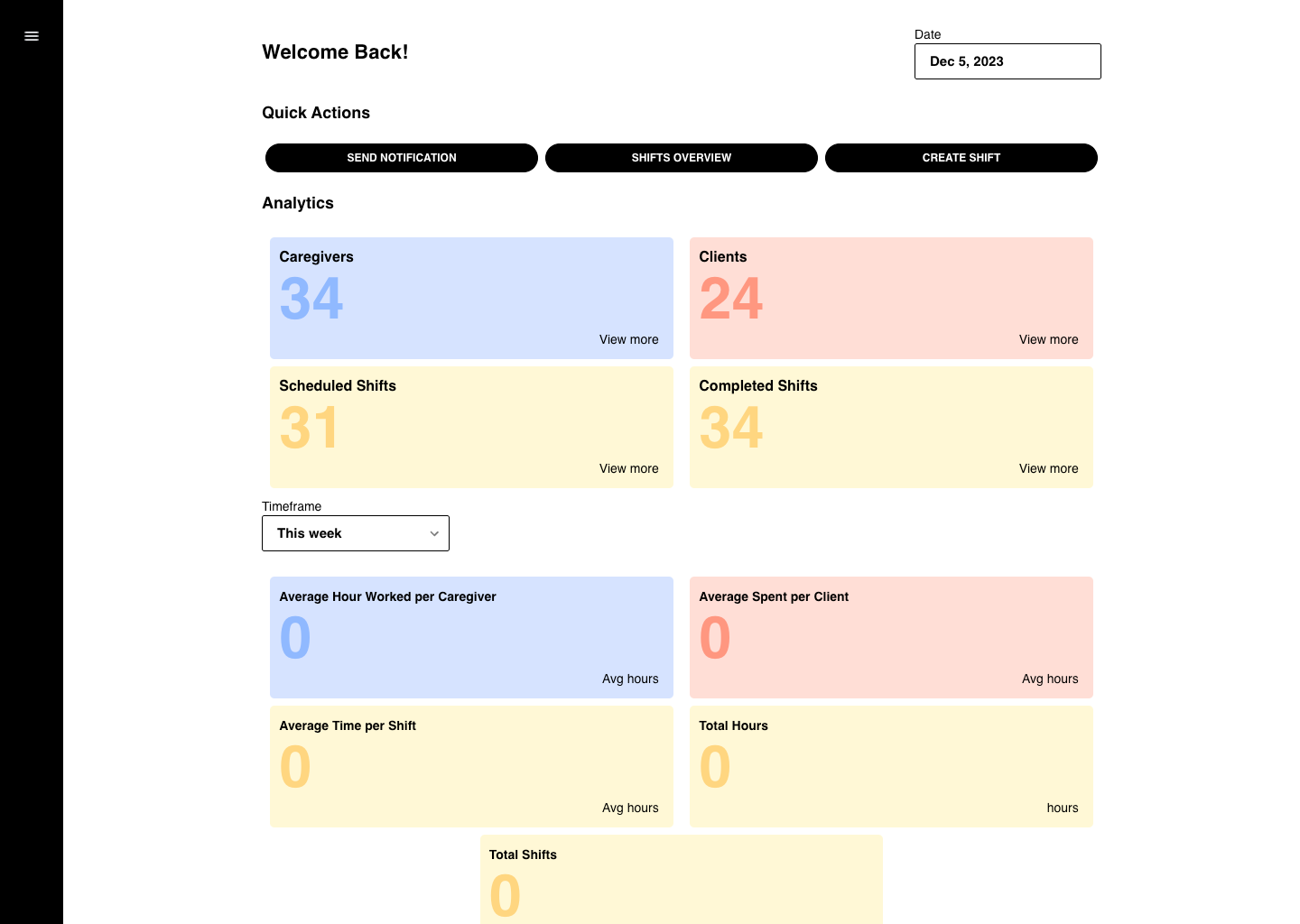
Original Build
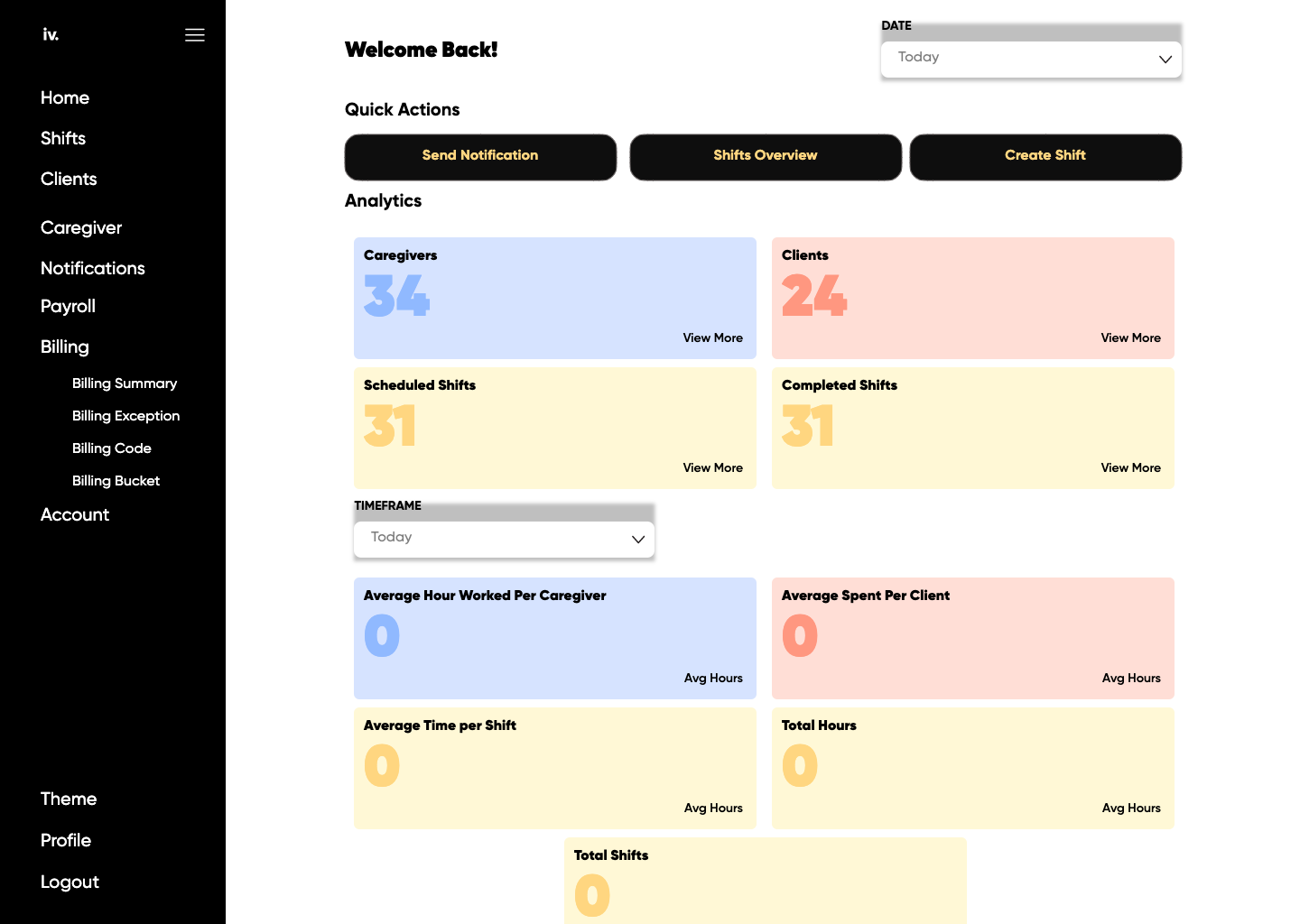
Beta Release
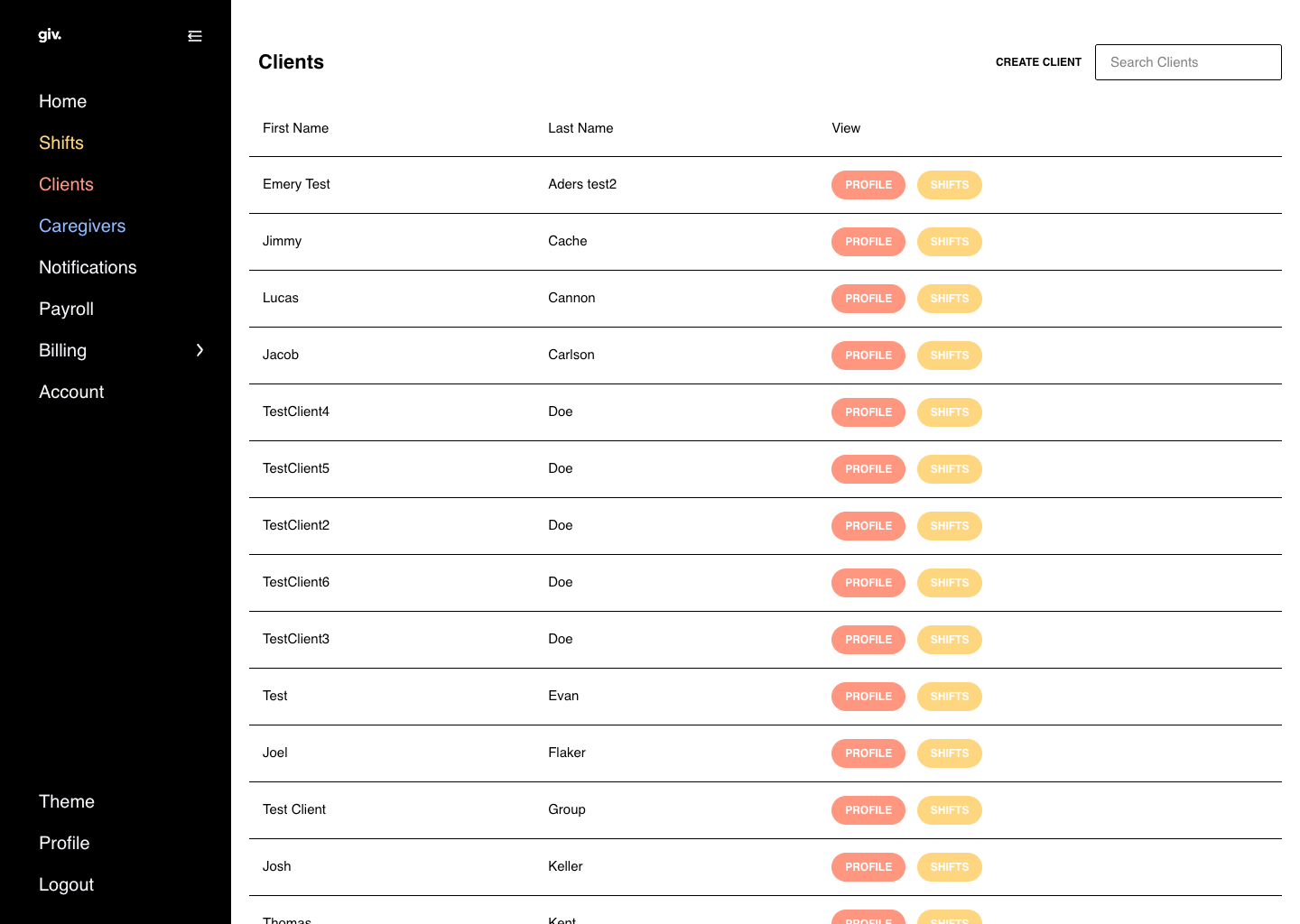
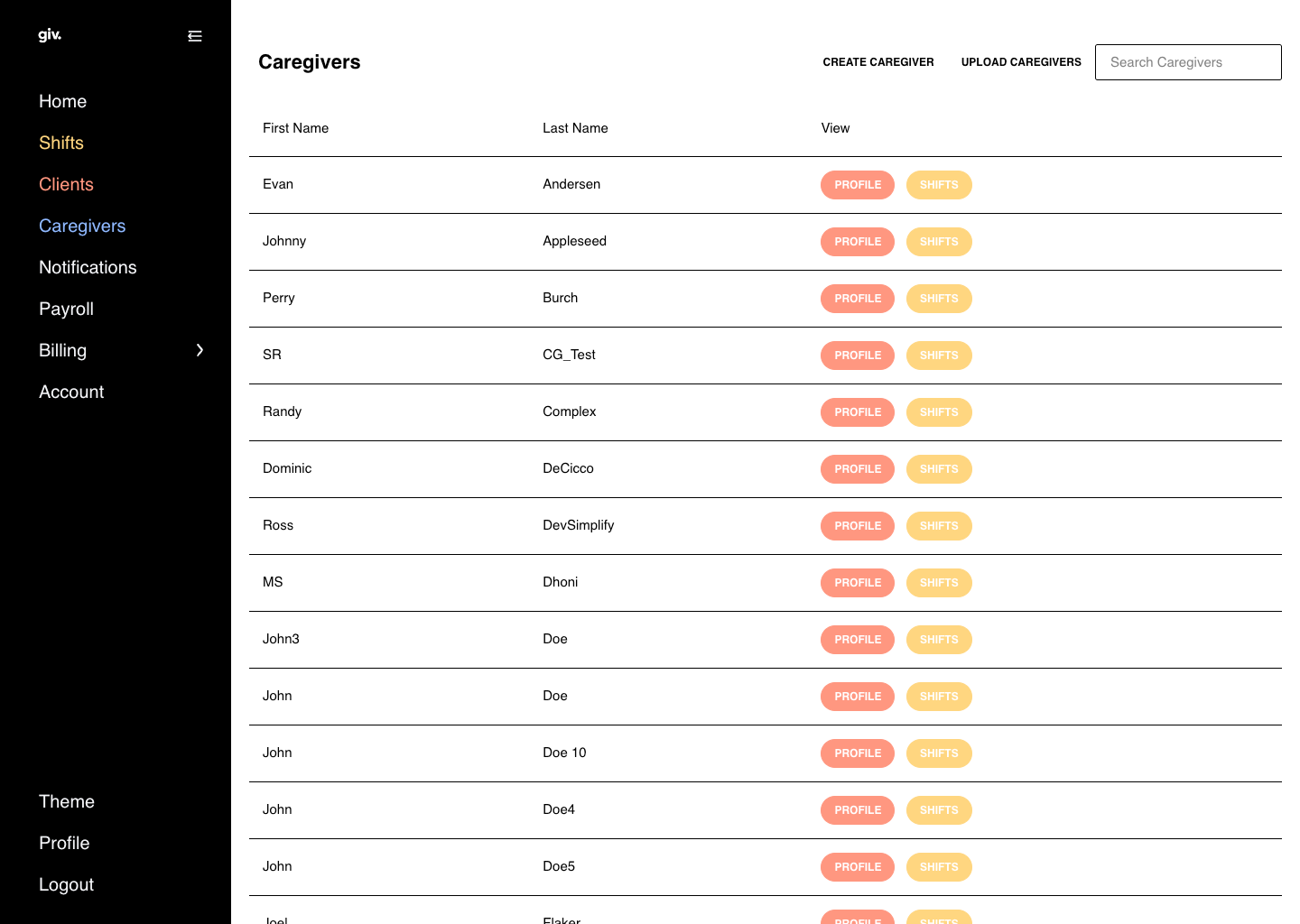
Current Platform
Project Details
- Client: Giv Healthcare
- Role: First and Lead UX/UI Designer
- Scope: Information architecture, UX flows, finished screens; scheduling, EHR, client and caregiver management, custom forms
- Platform: Web application (desktop)
- Related: Mobile App | Billing + Design System
- Live Product: givhealthcare.com
The Challenge
IDD agencies -- those supporting people with intellectual and developmental disabilities in group homes, supported living, and community care settings -- were managing some of the most complex care operations in healthcare using some of the least capable tools. Scheduling lived in spreadsheets. Caregiver records were on paper or in systems that shared nothing with each other. Shift notes were handwritten and stayed in a binder at the care site. Medication administration was tracked manually. Billing was handled in standalone software with no connection to the scheduling or documentation that generated the underlying data.
When a caregiver arrived for a shift, the information they needed about their client -- medications, behavioral triggers, goals, what kind of day the person had -- had to be verbally transferred from the outgoing caregiver or it was simply unavailable. In an industry with chronically high caregiver turnover, that knowledge gap was a patient safety risk dressed up as a software problem. Larger software companies had looked at the space and moved on: the complexity of IDD-specific Medicaid rules, state-by-state variation, and thin agency margins did not make for an attractive market. Giv decided to build anyway.
The Strategy
There was no PM at the start. The first task was to define, with the dev team, what the system actually needed to hold. The information architecture had to be mapped from the problem outward: what data existed across an agency's operations, how it connected, who needed to access what and when. The architectural principle that drove every decision was integration. A disconnected system would replicate the exact failure mode agencies were already living with. If scheduling and billing didn't share data, the billing automation that could make the product genuinely transformative would be impossible.
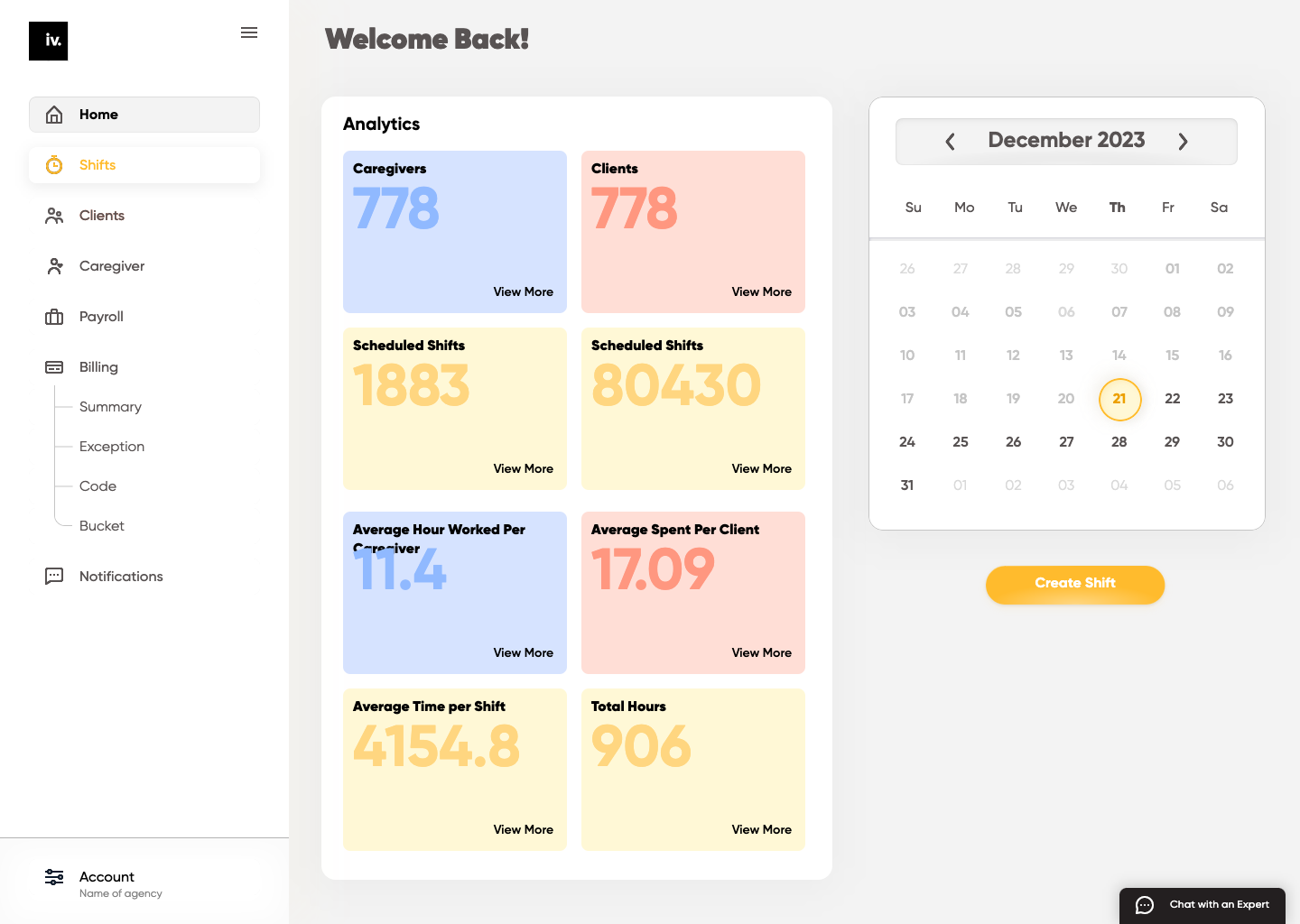
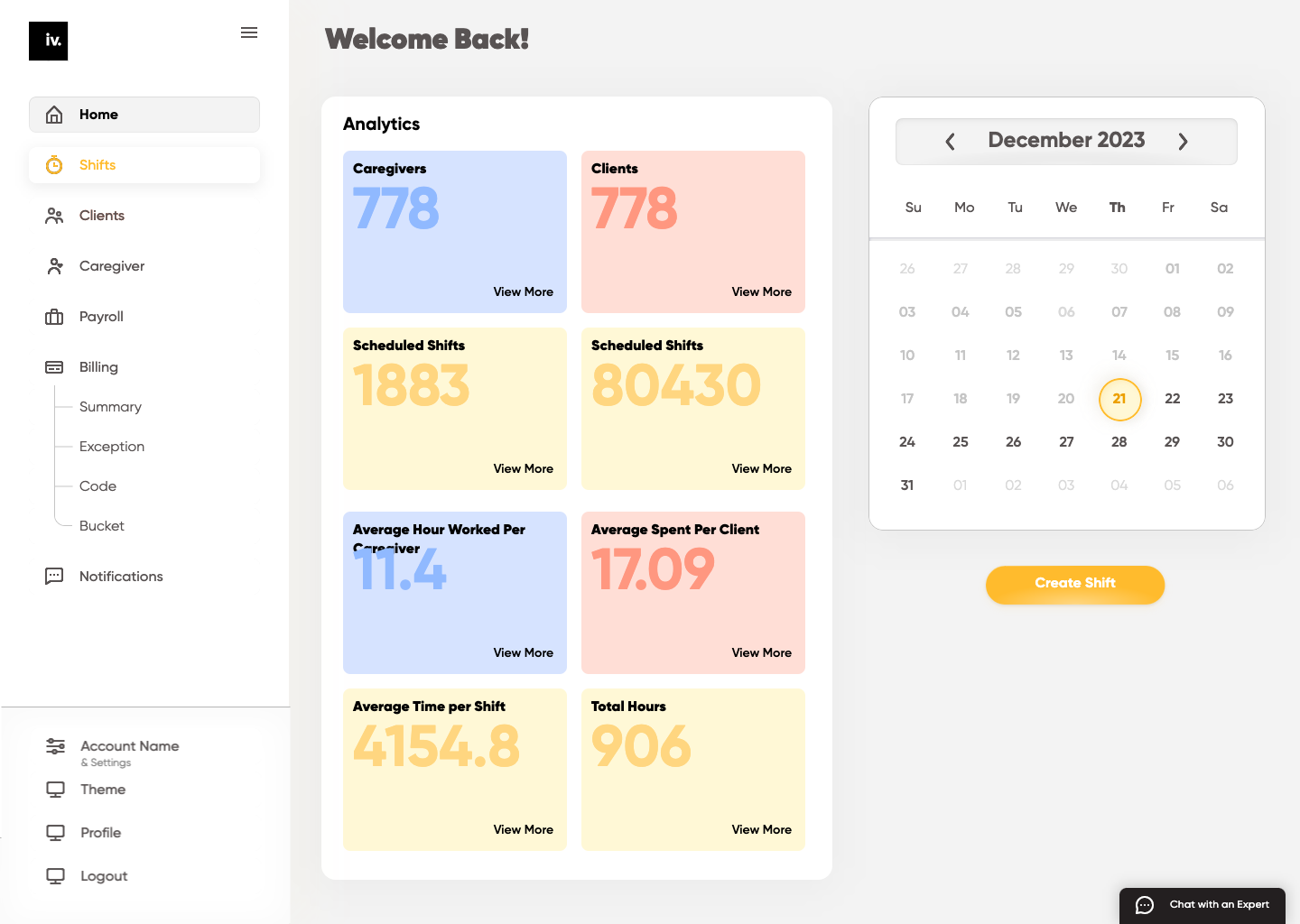
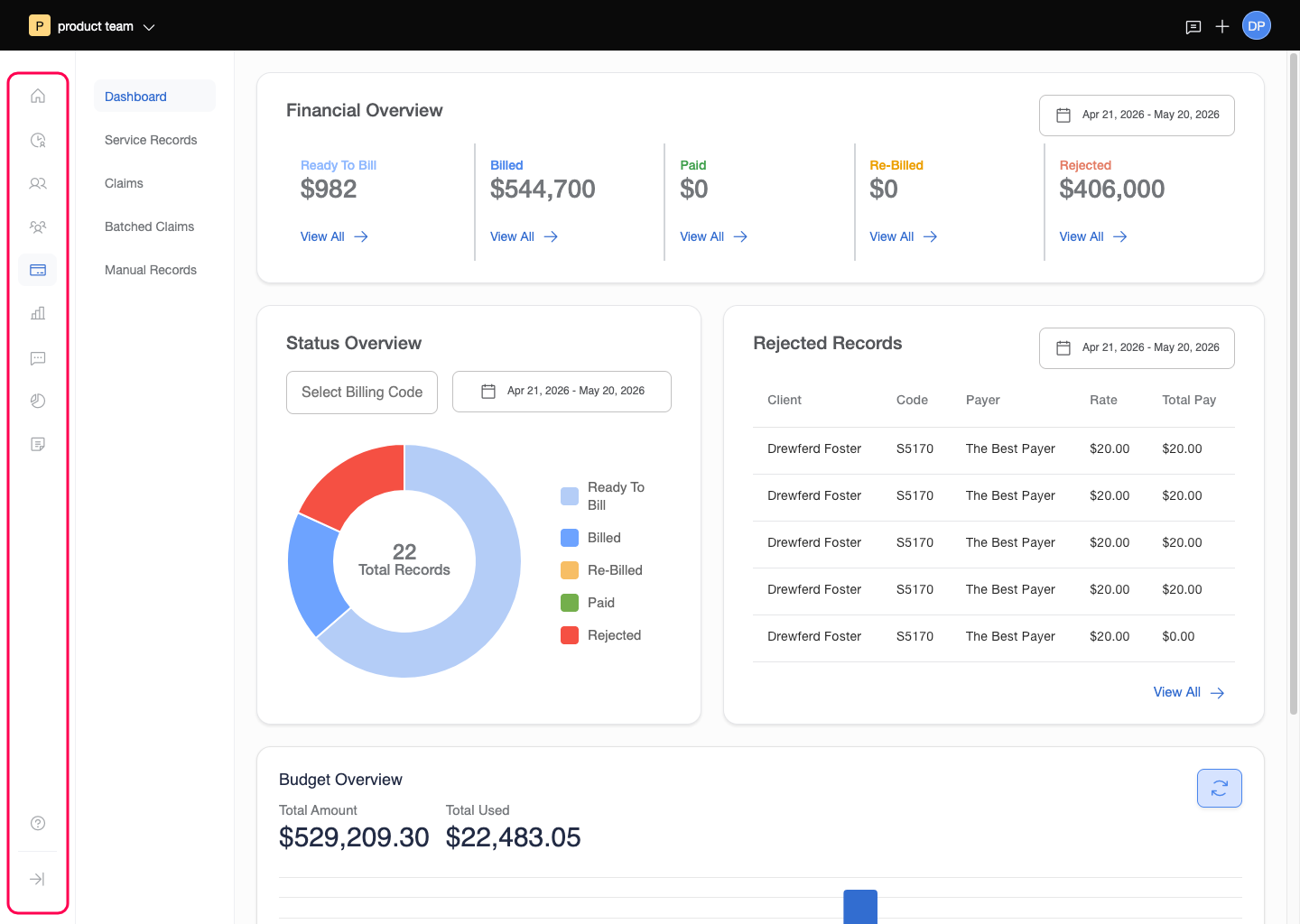
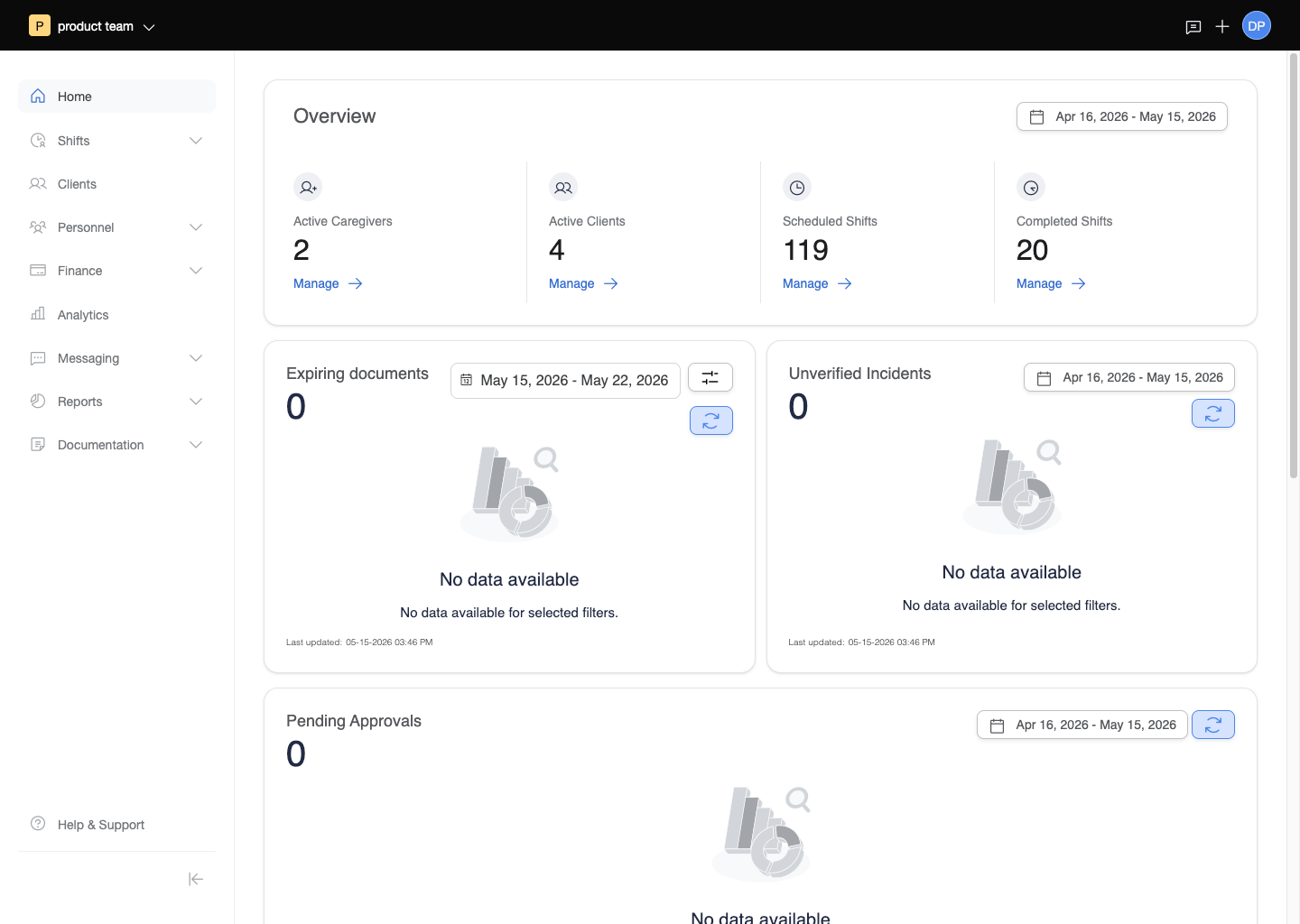
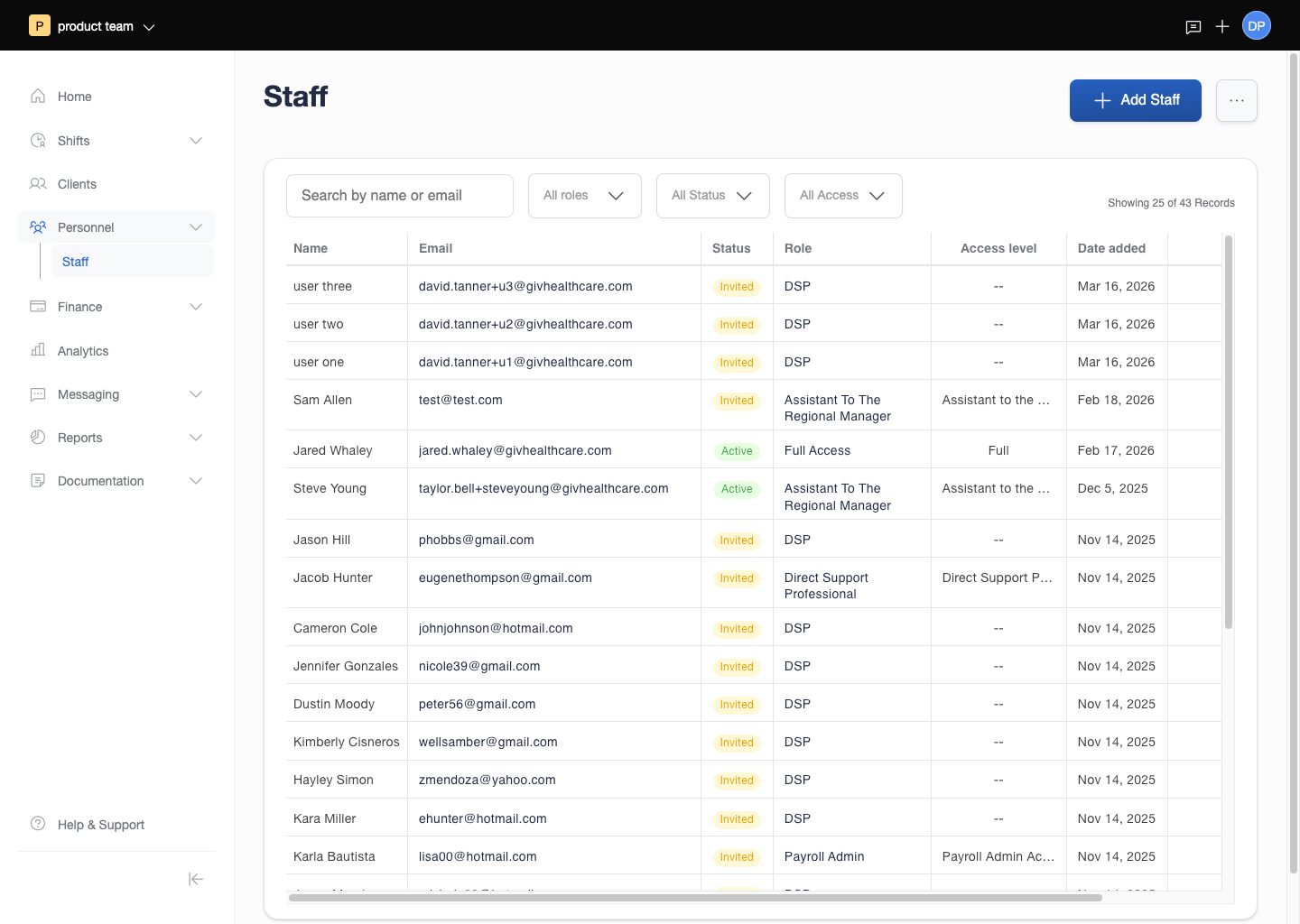
Five connected hubs emerged from that mapping: Client Hub (care profiles, EHR, eMAR, goals, behavioral notes), Staff Hub (caregiver records, certifications, availability), Scheduling Hub (shifts, assignments, coverage), Revenue Hub (billing, budgets, claims), and Reporting Hub (outcomes, compliance). Each hub was designed to pull from and feed into the others through shared data rather than through exports or manual entry.
The Execution
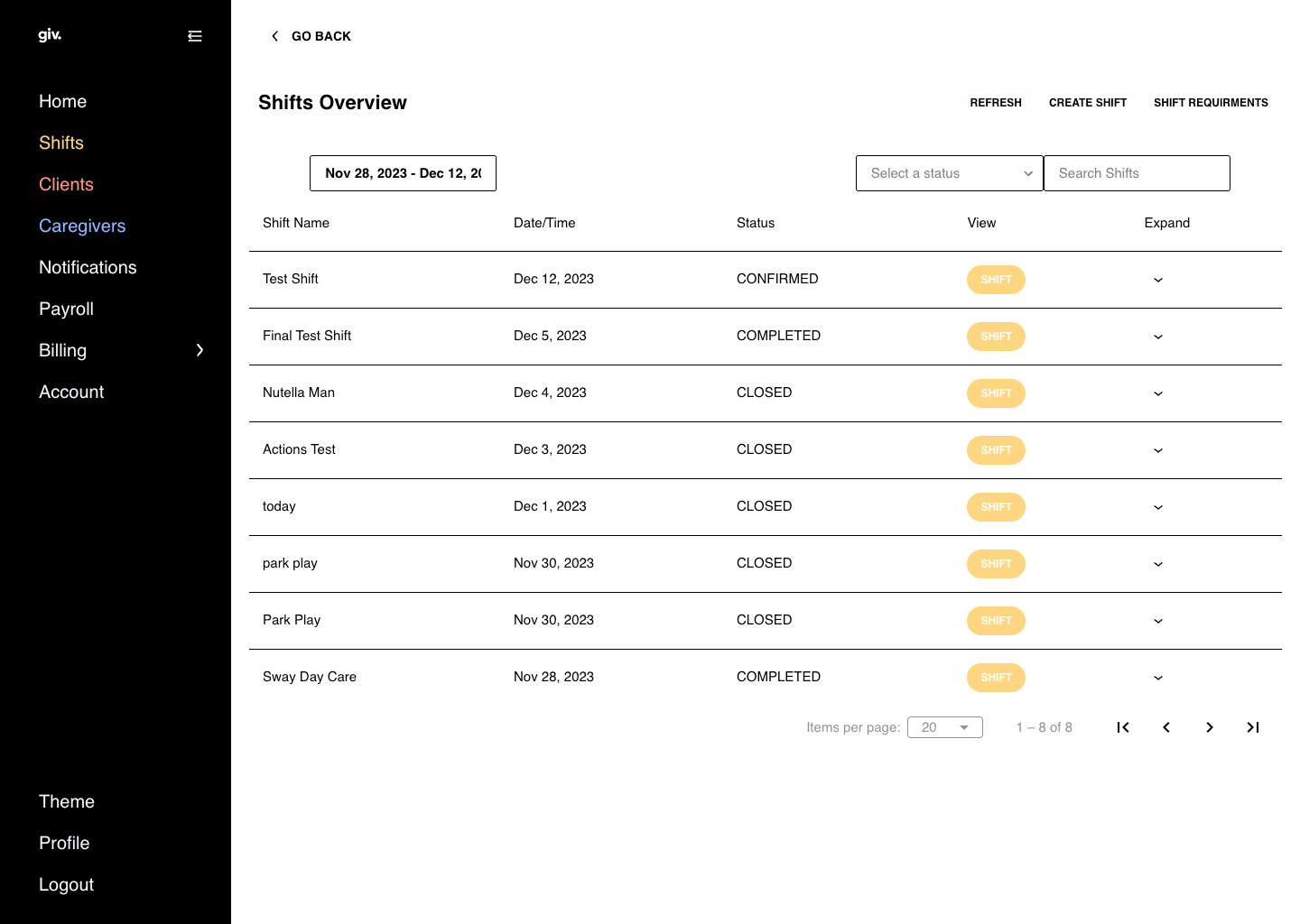
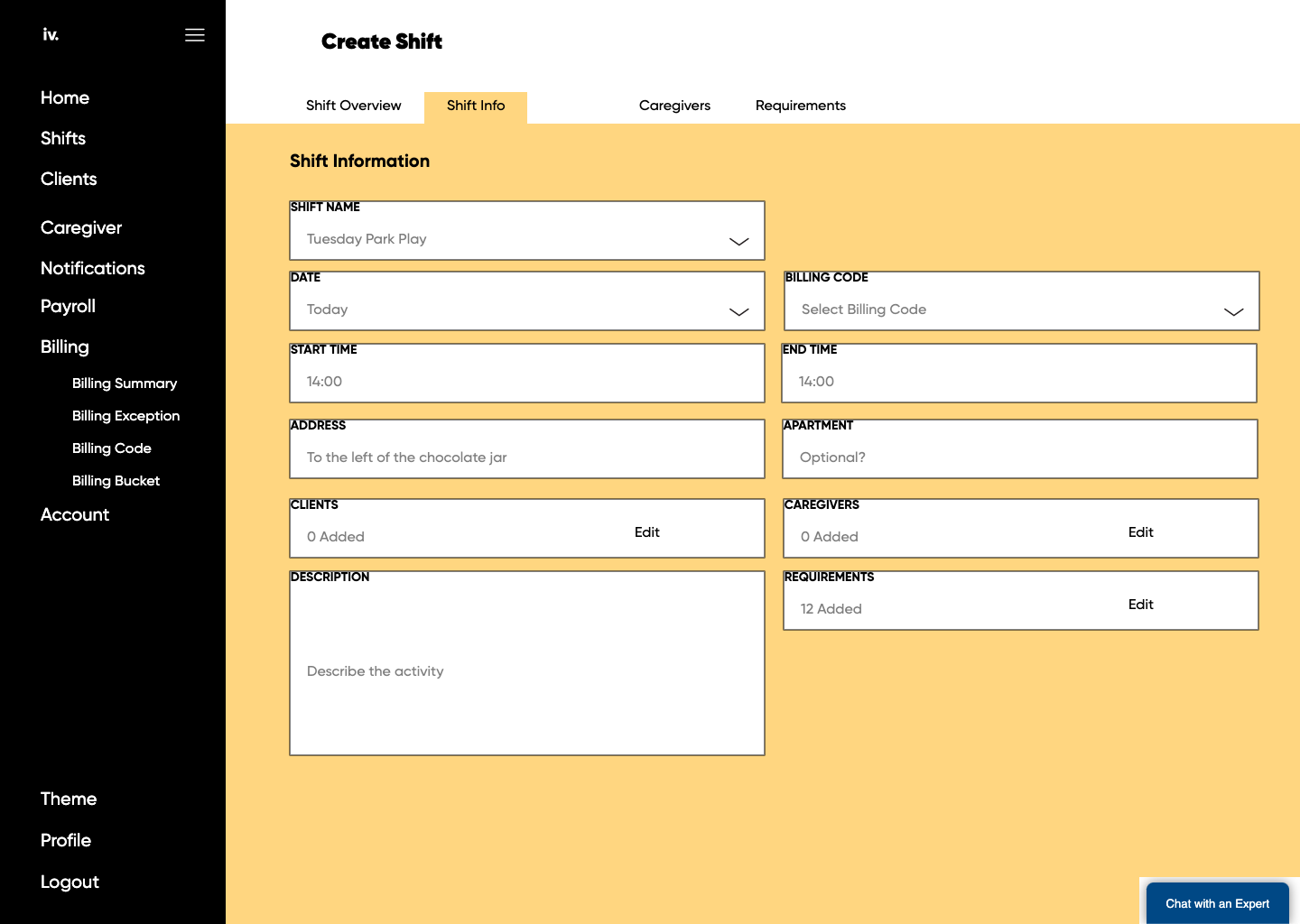
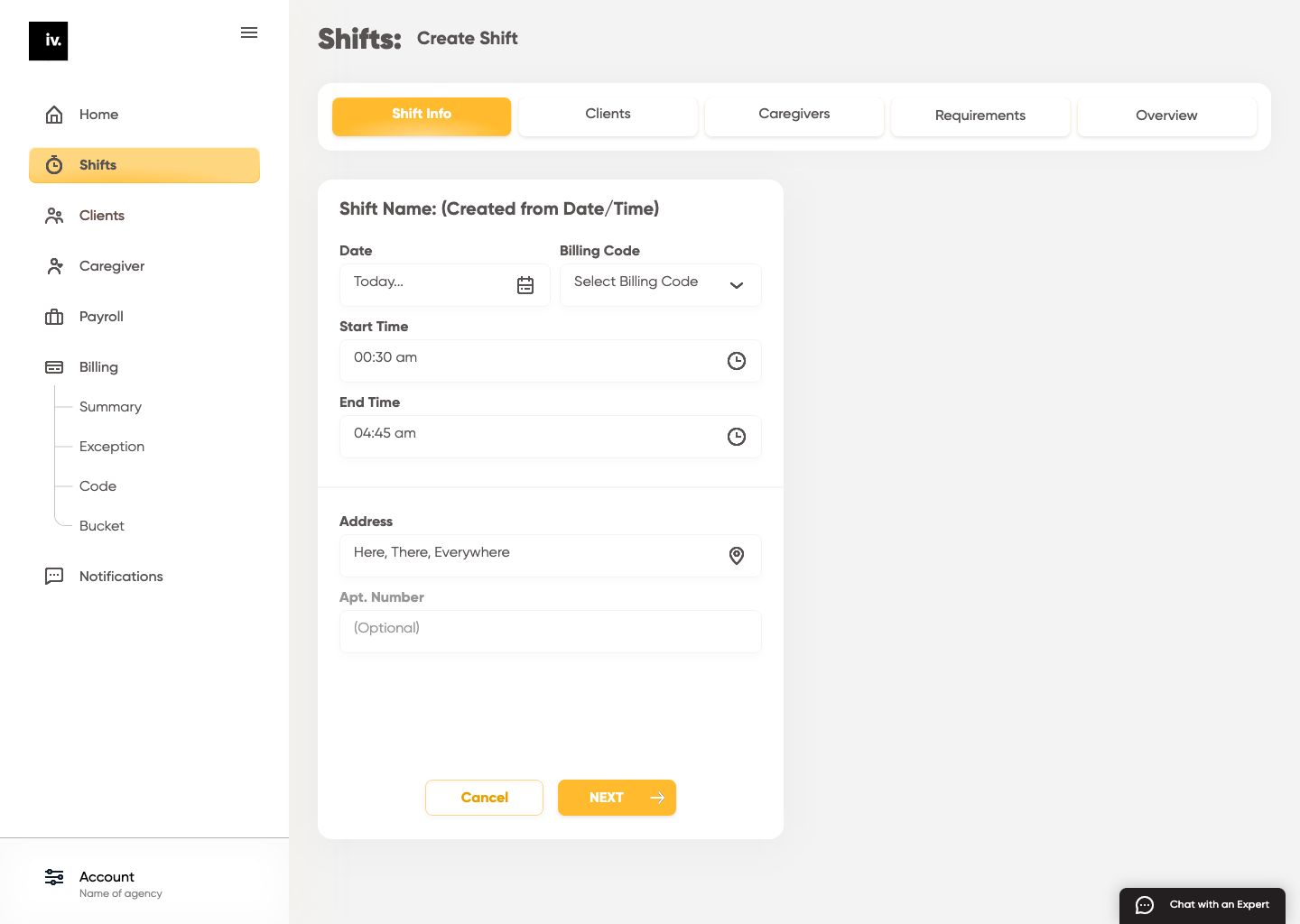
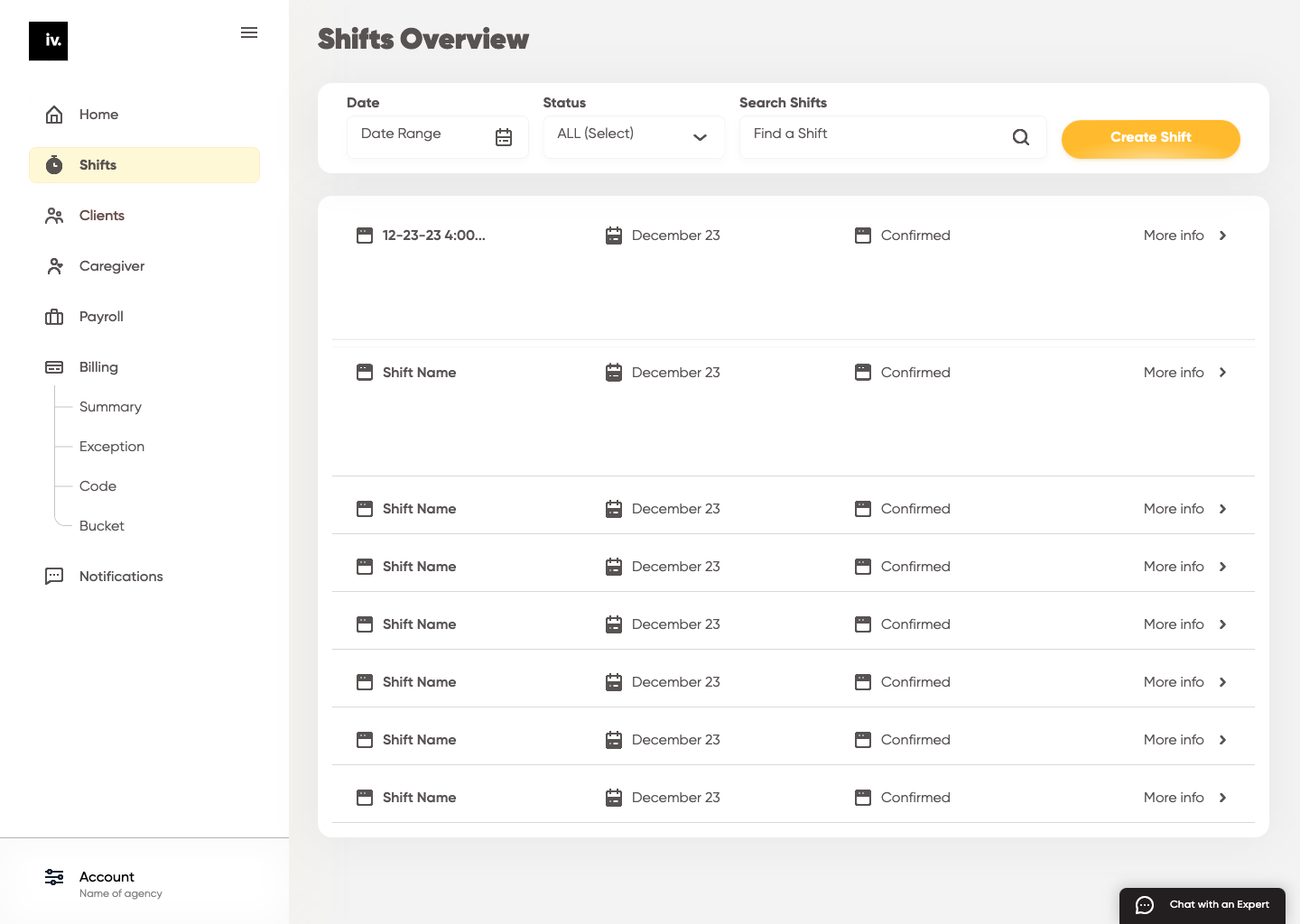
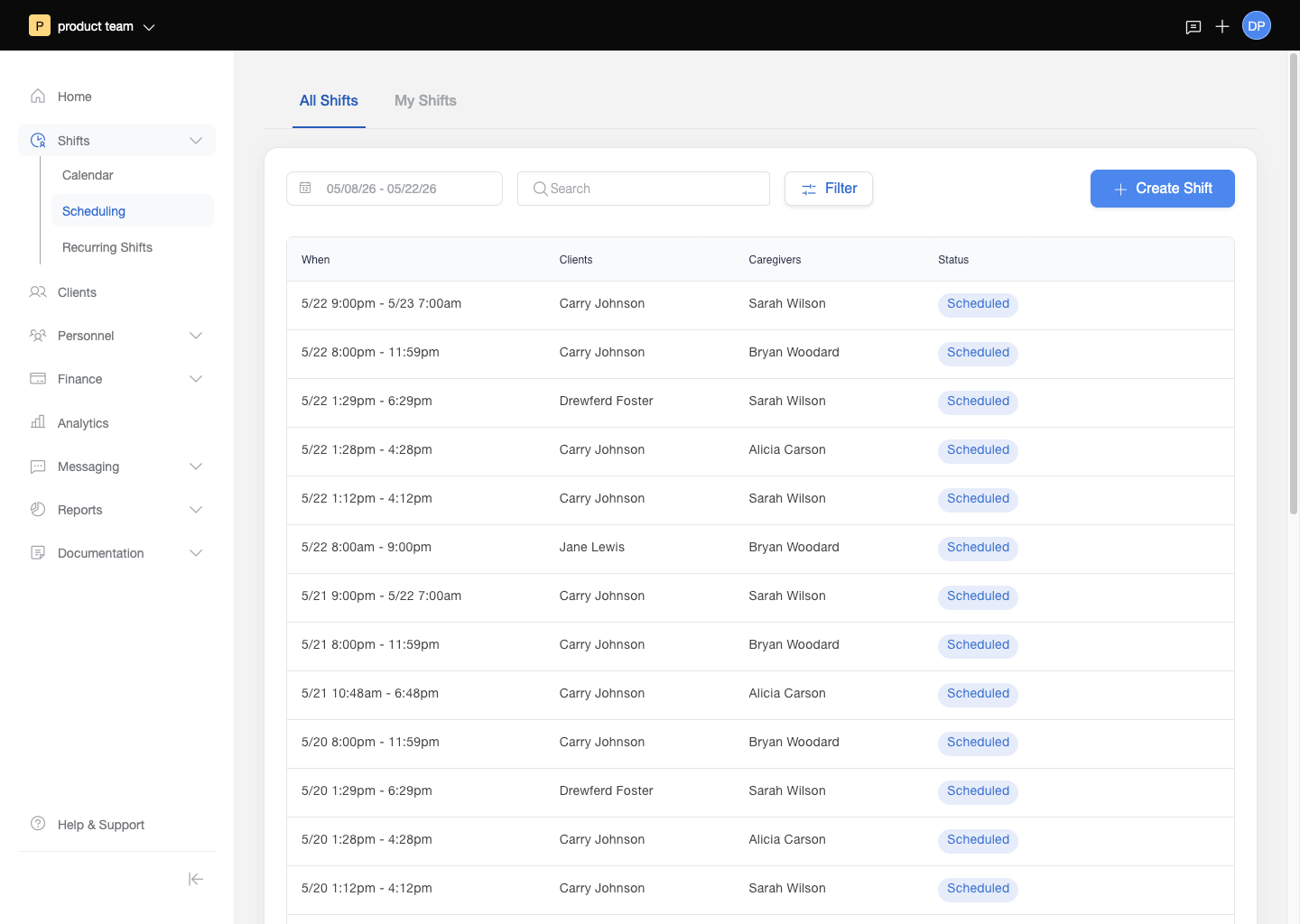
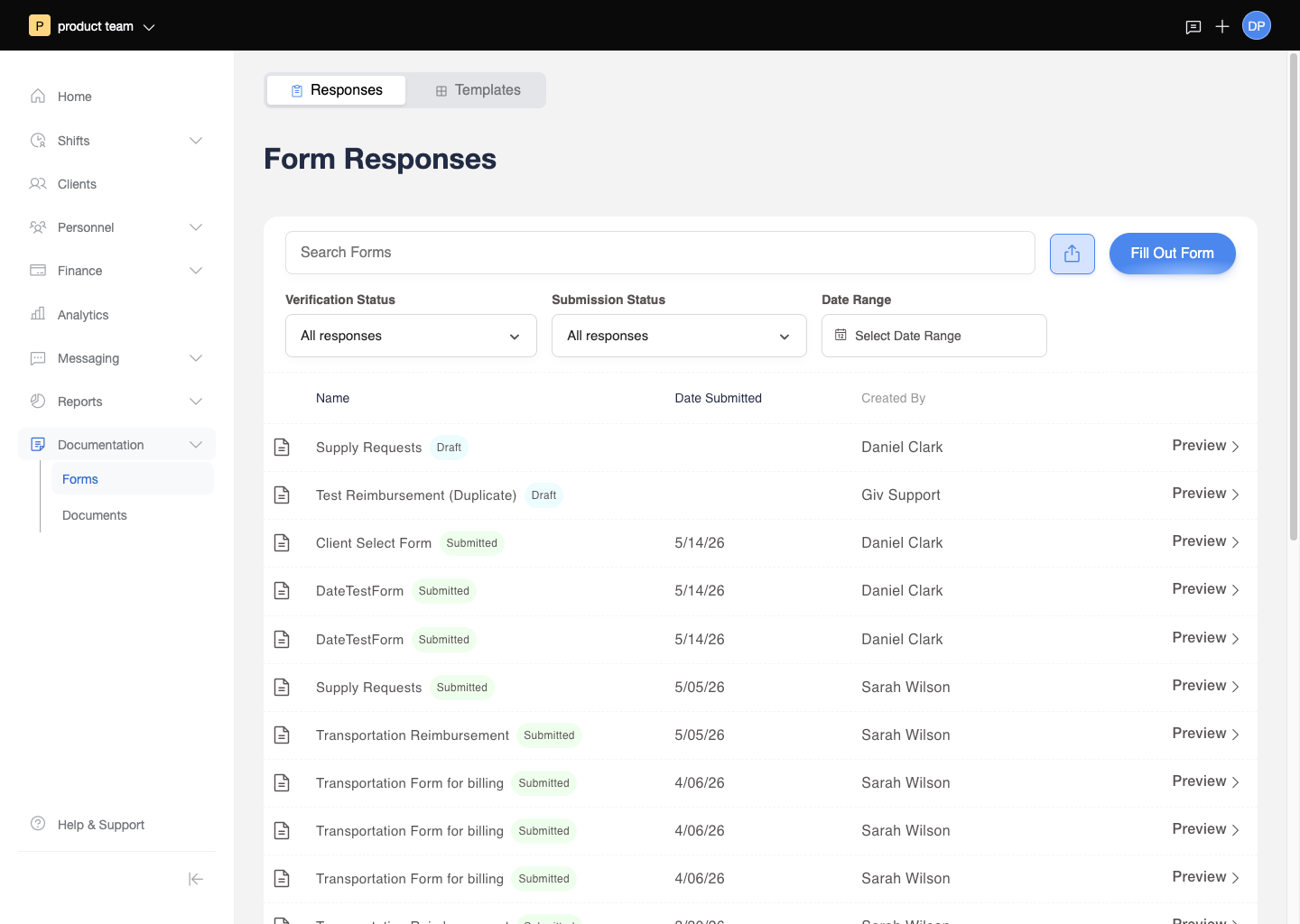
Flows were built for each module in sequence, with finished screens handed to the dev team for implementation. Scheduling came first -- it was the connective tissue everything else plugged into. Client profiles followed, then EHR and eMAR integration, then the shift documentation that DSPs (Direct Support Professionals) would complete in the field. When a PM joined, the work shifted from solo mapping to collaborative prioritization: what did agencies need immediately, what was dependent on earlier modules, and what could be phased in after the core system was stable.
The shift creation flow required particular care. It wasn't just a scheduling action -- it was the moment when compliance enforcement happened. Assigning a DSP to a client triggered certification checks. Adding a shift type triggered documentation requirements. The flow had to surface the right guardrails without turning every shift creation into a compliance exercise for the scheduler.
As Giv secured additional funding, the team grew from one to five, and three more designers joined. The design system that had started as a set of working patterns became a formal system. The work on the core platform handed off to a collaborative team, and the next phase of focused work began on billing.
The Results
The platform launched and grew. The all-in-one architecture that had been the founding design principle became Giv's primary market differentiator -- scheduling, billing, payroll, EHR, and eMAR in one system, with data flowing between them automatically. The Medicaid billing automation that became a key product feature was only possible because the shift documentation and scheduling data were already in the same database. The complexity that had made larger companies avoid IDD software was exactly what made Giv valuable to the agencies it served.